
Rise in Gender Dysphoria of Pressing Importance
After WYA’s 22nd International Solidarity Forum on the theme of Gender Ideology (which is defined as the insistence on a single idea or worldview as the only legitimate understanding of reality, rejecting all dissent), during which young members spent a week analyzing, assessing, and understanding how such ideology impacts children, families, and society, the topic continues to be of pressing importance.
In January, during the first 100 days, President Trump signed an Executive Order, Protecting Children From Chemical and Surgical Mutilation. The title sounded too transparently horrific and so was translated in headlines such as, “Trump Bans Gender-Affirming Care for Children.” Since then, this May, the United States Department of Health and Human Services published its Treatment for Pediatric Gender Dysphoria, reviewing the practices and guidelines put forth by WPATH (World Professional Association for Transgender Health). The Foreword of the Report states:
“The natural history of pediatric gender dysphoria is poorly understood, though existing research suggests it will remit without intervention in most cases… Nevertheless, the ‘gender-affirming’ model of care includes irreversible endocrine and surgical interventions on minors with no physical pathology.”
According to a Reuters investigation entitled, A Dearth of Science, “[p]uberty blockers and sex hormones do not have U.S. Food and Drug Administration (FDA) approval for children’s gender care. No clinical trials have established their safety for such off-label use… And in 2016, the FDA ordered makers of puberty blockers to add a warning about psychiatric problems to the drugs’ label after the agency received several reports of suicidal thoughts in children who were taking them.”
Attempted “Guidelines” to Affirm Gender Dysphoria
The current approach to treating pediatric gender dysphoria follows the “gender-affirming” model of care recommended by the World Professional Association for Transgender Health (WPATH). This model is also endorsed by the Endocrine Society. Note that all but one of the authors of the Endocrine Society Clinical Practice Guidelines published in 2017 were not just affiliates of WPATH but board members, one researcher was a former President of WPATH and others were committee members.
The treatment follows the pattern of social transition (changing name and pronouns, dressing like the preferred gender), puberty blockers starting as young as 10, cross-sex hormones during adolescence and surgery. These “gender affirming” interventions are framed as safe — and reversible. Neither of these claims are true, as puberty is a rapid time of growth and development of the brain and every system of the body, and cannot be “redone” once missed. Giving children and adolescents puberty blockers and cross-sex hormones poses irreparable risks and harms including “…infertility/sterility, sexual dysfunction, impaired bone density accrual, adverse cognitive impacts, cardiovascular disease and metabolic disorders, psychiatric disorders, surgical complications, and regret.”
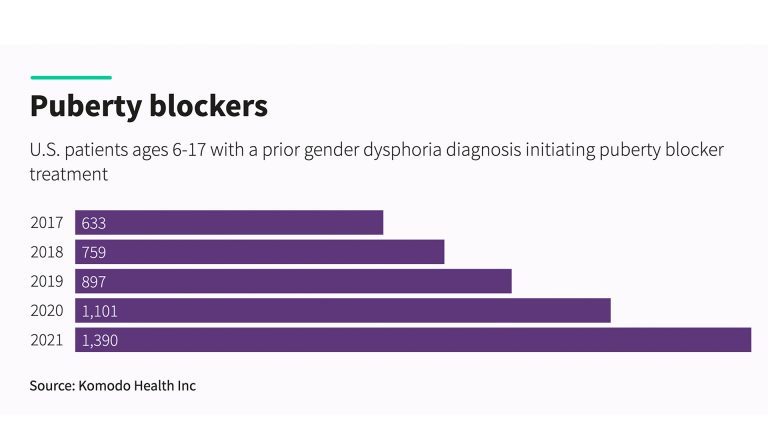
While many firmly believe that medical decisions for minors are made in consultation with parents or guardians and only after rigorous and thorough multidisciplinary assessments, statistics and the lived experiences of many do not support this claim. In the HHS Report, pediatric endocrinologist, Daniel Shumer, of the Comprehensive Gender Services Program (CGSP) at University of Michigan Health, confirms that medicalization is the norm rather than the exception, as the greater majority of pediatric patients referred to his clinic end up receiving cross-sex hormones. Gender dysphoria statistics are alarming, considering the diagnosis of Gender Dysphoria in children ages 6–17 in the US is surging, with a reported 70% increase from 2017–2021.
In the Standards of Care 8th Version, WPATH seeks to address: “Medically necessary gender-affirming interventions” which include but are not limited to: “hysterectomy +/- bilateral salpingo-oophorectomy; bilateral mastectomy, chest reconstruction or feminizing mammoplasty, nipple resizing or placement of breast prostheses; genital reconstruction, for example, phalloplasty and metoidioplasty, scrotoplasty, and penile and testicular prostheses, penectomy, orchiectomy, vaginoplasty, and vulvoplasty; hair removal from the face, body, and genital areas for gender affirmation or as part of a preoperative preparation process; gender-affirming facial surgery and body contouring; voice therapy and/or surgery; as well as puberty blocking medication and gender-affirming hormones; counseling or psychotherapeutic treatment as appropriate for the patient and based on a review of the patient’s individual circumstances and needs.”
It is well established in research that the majority of children and adolescents struggling with gender dysphoria have co-occurring psychiatric or neurodevelopmental conditions that make them especially vulnerable. However, “counseling or psychotherapeutic treatment” is not first but last on the list of interventions recommended by WPATH.
WPATH’s Controversial History
Before this, WPATH was formerly called the Harry Benjamin International Gender Dysphoria Association. Harry Benjamin was a friend of Alfred Kinsey, a controversial American sexologist. In a New York Times article, Benjamin describes Kinsey as an “old friend of mine and a great man.” Following the theme of controversy, Benjamin had been administering cross-sex hormones and radiation to sterilize patients for decades. In 1949, Kinsey referred a patient to Benjamin, and from this close friendship emerged some of the first documented cases of giving cross-sex hormones to children in the US.
The Kinsey Institute, based out of the University of Indiana, considers itself “the trusted source for critical issues in sexuality, gender, and reproduction.” Despite calling itself a “trusted source,” in the 1948 book, Sexual Behavior in the Human Male, Kinsey horrifyingly shows tables illustrating pre-adolescent children’s orgasms, in boys from the age of two months to 15 years. In Kinsey’s own words, children’s orgasms were measured based on their “groaning, sobbing, or more violent cries, sometimes with an abundance of tears.” (Citations located below).
Benjamin also worked with the urologist, Elmer Belt, who performed the surgeries for his patients, and in their growing fear of legal reprisal, Benjamin developed the first Standards of Care Protocol to include sending the patient for psychiatrist assessment. As Benjamin wrote to Belt in a letter, “I understand your hesitation to operate, although the psychiatric evaluation would protect you.” In 1966, the publication of Benjamin’s book, The Transsexual Phenomenon, coincided with the opening of the John Hopkins Gender Clinic, where Dr. John Money would castrate 18-month-old Bruce Reimer, create a rudimentary vulva, call him Brenda, and insist that Bruce be socialized as a girl. Money reported on the case as a success, but ‘Brenda’ struggled throughout his life and eventually committed suicide. Milton Diamond wrote an exposé and journalist John Colapinto wrote a book on the subject: As Nature Made Him: The Boy Who was Raised as a Girl.
As if this were not bad enough, in a New York Times article, it is detailed that Kinsey had written to a 63-year-old pedophile, Rex King, and coaxed him to “send his detailed diaries of his sexual exploits, including those with children.” Kinsey met with the pedophile, and later published much of his “data” in the book, attributing it not to any one source but as representative of the average male. Years later, John Bancroft, a former director of the Kinsey Institute “discovered” that all the data came from the pedophile, King. However, this fact was known at the time, as Kinsey’s co-author, Paul Gebhard, admitted to interviewers that the criminality of the work was known and that they failed to “cooperate with authorities in apprehending a pedophile we had interviewed who was being sought for a sex murder.”
Where “Guidelines” Stand Today
As the US Treatment for Pediatric Gender Dysphoria Report states, the purported benefits of medical interventions are fraught with controversy and the “reviews of the evidence have revealed deep uncertainty about the purported benefits of these interventions.” It calls attention to the fact that in a recent systematic review of international guideline quality, neither WPATH nor the Endocrine Society Clinical Practice Guidelines are recommended for clinical use as they “lack developmental rigour and transparency.”
Even more, the Report exposes the fact that WPATH suppressed systematic reviews that it “…believed would undermine its favored treatment approach…” and that WPATH “violated conflict of interest management requirements and eliminated nearly all recommended age minimums for medical and surgical interventions in response to political pressures.”
Whistleblower, Jamie Reed, who spoke at the 22nd International Solidarity Forum on Gender Ideology, and Dr. Eithan Haim, who spoke at last year’s Forum on Human Dignity and Totalitarian Ideologies, are both featured in the Report, amongst others who have had firsthand experience with working behind the scenes in gender clinics and with gender dysphoria symptoms. The outcomes of social transition, puberty blockers, and cross-sex hormones, is abundantly clear: there is little quality evidence to corroborate the idea that any of these interventions improve mental health outcomes over any given period of time.
The Report furthers, “[h]aving recognized the experimental nature of these medical interventions and their potential for harm, health authorities in a number of countries have imposed restrictions.” For example, after the 2024 UK Cass Review (a comprehensive, independent review commissioned by NHS England) was published, “the UK has banned the routine use of puberty blockers as an intervention for pediatric gender dysphoria.” The author, Dr. Hilary Cass, stated in an interview, “I certainly wouldn’t want to embark on a treatment where somebody couldn’t tell me with any accuracy what percentage chance there was of it being successful, and what the possibilities were of harms or side effects.”
Perhaps this is why WPATH recognizes that “health is not only dependent upon high-quality clinical care…” and seeing the writing on the wall with regards to the scientific inefficacy of its proposed medical interventions, WPATH is committed to advancing “…public policies and legal reforms…” as well.
Finally, the Treatment for Pediatric Gender Dysphoria Report concludes that, “there was a rapid expansion and implementation of a clinical protocol that lacked sufficient scientific and ethical justification. Second, when confronted with compelling evidence that this protocol did not deliver the health benefits it promised…medical professionals and associations failed to reconsider the ‘gender-affirming’ approach.”
We at World Youth Alliance commend all courageous medical doctors and researchers who prioritize scientific findings and children’s health over ideology, and will continue to investigate as necessary to report the truth of the human person to all audiences.
(The cover image attached is courtesy of the article, Putting numbers on the rise in children seeking gender care)
Citations:
Kinsey, Alfred, Sexual Behavior in the Human Male, Indiana University Press, 161 (1948).
William H. Masters, Virginia E. Johnson, Robert C. Kolodny, Ethical Issues in Sex Therapy and Research, Boston, Massachusetts: Little, Brown and Company, 13 (1977).


